Individual air cells deflate to protect patient's vulnerable areas in prone position
Treating ARDS with Prone Position Ventilation
Prone position ventilation is proven to provide substantial clinical benefits to patients with moderate or severe acute respiratory distress syndrome (ARDS) (PaO2/FiO2≦200 mmHg). Patients treated in a prone position during mechanical ventilation are usually in a prone position for prolonged periods >12 hours per day1. According to various published clinical studies, prone position ventilation could improve oxygenation through more uniform distribution of blood flow/airflow for ARDS patients2.
Excessive pressure to vulnerable areas increases pressure injury risks and recovery time
Prone positioning significantly increases pressure injury risk in vulnerable areas. Non-optimized pressure distribution system applies excessive pressure to vulnerable areas such as the patient's face, ears, shoulder, chest, genitalia, iliac crests and anterior leg region, resulting in a higher risk of pressure injury complications and longer recovery3. The original clinical practice was that to further reduce the pressure exerted on breasts, abdomen, or knees, a caregiver team lifts the patient's chest, pelvis, or chin to insert pillows. Lacking proper tools for caregivers to keep track of pressure settings for different regions of the support surface increases the burden on the caregiver's workload.
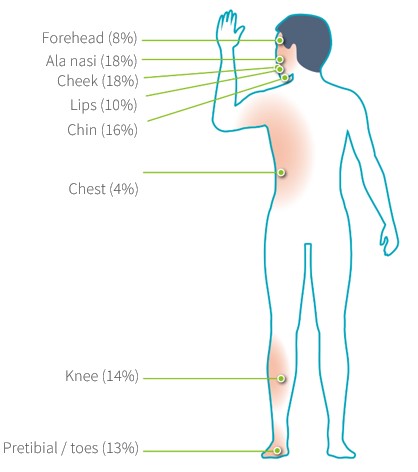
Figure1:Topographic distribution of pressure sores by location
Protect patient's vulnerable areas
It allows the caregivers to customize the pressure-relief area based on patient’s body contour, height, and clinical condition, to optimize pressure injury prevention effect.
Control over individual air cell airflow allows zero pressure and personalized care to vulnerable areas, preventing pressure-induced injuries and avoiding excess pressure in the abdomen area to improve respiratory system function.
 Figure2:Deflate individual air cell to protect vulnerable areas
Figure2:Deflate individual air cell to protect vulnerable areas
References:
1. Fan, Eddy et al. “An Official American Thoracic Society/European Society of Intensive Care. Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome.” American journal of respiratory and critical care medicine vol. 195,9 (2017): 1253-1263. doi:10.1164/rccm.201703-0548ST
2. Pelosi, P et al. “Prone position in acute respiratory distress syndrome.” The European respiratory journal vol. 20,4 (2002): 1017-28. doi:10.1183/090319 36.02.00401702
3. Ibarra G, Rivera A,
Fernandez-Ibarburu B, Lorca-García C, Garcia-Ruano A. Prone position pressure
sores in the COVID-19 pandemic: The Madrid experience. Journal of Plastic,
Reconstructive & Aesthetic Surgery : JPRAS. 2021 Sep;74(9):2141-2148. DOI:
10.1016/j.bjps.2020.12.057. PMID: 33446462; PMCID: PMC7837206.
